RE: Docket #: DHS-2004-0029 Docket #: Z-RIN 1660-ZA02
To: Rules Docket
Clerk,
I am a retired diagnostic radiologist and
I am submitting this comment regarding Protective Action
Guidelines for Radiologic Disperal Device (RDD) and Improvised Nuclear Device
(IND).
We are all familiar with the idea that
there can be too much of a good thing. A perfect example is HIPPAA, the end
product of a massive over-reaction to privacy concerns that impedes vital
communication between physicians and hospitals, creates Kafka-esque volumes of
paperwork and serves as a monstrous time, energy and cost sink (We even had to
create a Compliance Officer for our medical group to 'enforce' and document
our privacy policy).
You can see where I'm heading: Like
privacy safeguards, radiation protection can exceed the point of diminishing
returns. Specifically, in the event of the explosion/dispersal of a
radioactive device, if an exaggerated concern for radiation exposure prevents
the rescue of injured victims---including self-rescue---or other emergency
measures such as fire suppression, or if it creates unwarranted long term
geographic, physical or psychological impairment, then it has clearly done
more harm than good.
Michael Crichton (
http://www.crichton-official.com/ ) puts it far better than I can in a 2005
article entitled, "Fear, Complexity and Environmental Management in the 21st
Century":
"Some of you know
I have written a book that many people find controversial. It is
called State of Fear, and I
want to tell you how I came to write it. Because up until five years ago, I
had very conventional ideas about the environment and the success of the
environmental movement.
The book really
began in 1998, when I set out to write a novel about a global disaster. In the
course of my preparation, I rather casually reviewed what had happened in
Chernobyl,
since that was the worst manmade disaster in recent times that I knew
about.
What
I discovered stunned me. Chernobyl was a tragic event, but nothing
remotely close to the global catastrophe I imagined. About 50 people had
died in Chernobyl, roughly the number of Americans
that die every day in traffic accidents. I don't mean to be gruesome,
but it was a setback for me. You can't write a novel about a global disaster
in which only 50 people die.
Undaunted, I began to research
other kinds of disasters that might fulfill my novelistic requirements.
That's when I began to realize how big our planet really is, and how resilient
its systems seem to be. Even though I wanted to create a fictional catastrophe
of global proportions, I found it hard to come up with a credible
example. In the end, I set the book aside, and wrote Prey instead.
But the shock that
I had experienced reverberated within me for a while. Because what I had
been led to believe about Chernobyl was not merely wrong-it was
astonishingly wrong. Let's review the
data.
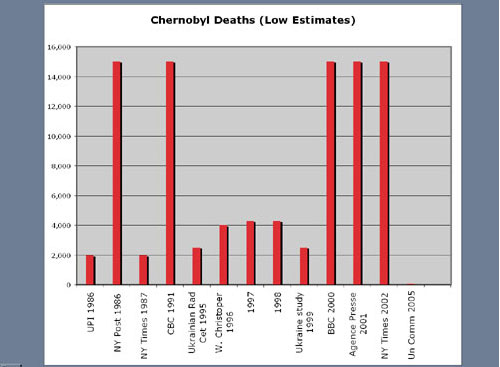
The
initial reports in 1986 claimed 2,000 dead, and an unknown number of future
deaths and deformities occurring in a wide swath extending from
Sweden to the Black Sea. As the years passed, the size of the disaster
increased; by 2000, the BBC and New York Times estimated 15,000-30,000 dead,
and so on·
Now, to report
that 15,000-30,000 people have died, when the actual number is 56, represents
a big error....But, of course, you think, we're talking about radiation: what
about long-term consequences? Unfortunately here the media reports are
even less accurate.
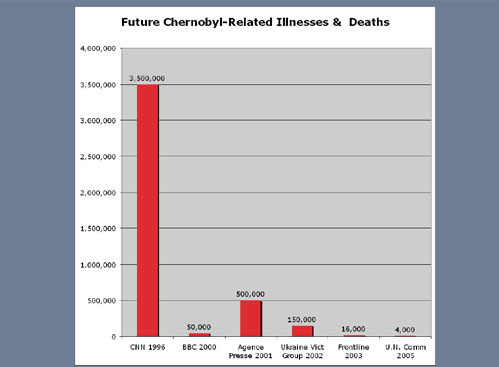
The chart
shows estimates as high as 3.5 million, or 500,000 deaths, when the actual
number of delayed deaths is less than 4,000. That's the number of
Americans who die of adverse drug reactions every six weeks. Again, a huge
error.
But
most troubling of all, according to the UN report in 2005, is that "the
largest public health problem created by the accident" is the "damaging
psychological impact [due] to a lack of accurate
information·[manifesting] as negative
self-assessments of health, belief in a shortened life expectancy, lack of
initiative, and dependency on assistance from the
state."
In
other words, the greatest damage to the people of Chernobyl was caused by
bad information. These people weren't blighted by radiation so much as by
terrifying but false information. We ought to ponder, for a minute,
exactly what that implies. We demand strict controls on radiation because it
is such a health hazard. But Chernobyl suggests that false information can
be a health hazard as damaging as radiation. I am not saying radiation is not
a threat. I am not saying Chernobyl was not a genuinely serious
event.
But thousands of
Ukrainians who didn't die were made invalids out of fear. They were told to be
afraid. They were told they were going to die when they weren't. They were
told their children would be deformed when they weren't. They were told they
couldn't have children when they could. They were authoritatively promised a
future of cancer, deformities, pain and decay. It's no wonder they responded
as they did."
I have also been in communication with my
physician colleague, Dr Jane Orient, and I am in complete agreement with her
view that, in the event of a terrorist attack using a nuclear device, we
should not apply the same radiation exposure limits that are appropriate in a
peacetime nuclear accident. In the interests of clarity, I would like to quote
from her earlier comments to you as
follows:
As the department recognizes, doses
above 5 rems may be unavoidable. It should also be recognized that doses
less than 100 rems are unlikely to lead to any acute symptoms. Indeed, a
significant long-term increase in death rates of atomic bomb survivors has
been shown only for those receiving doses greater than about 200 rads. (See
Kondo S, Health Effects of Low-Level
Radiation, Medical Physics Publishing, Madison, Wis., 1993).
Indeed, at "low" or "intermediate" levels of exposure, there was apparently a
beneficial effect on longevity.
The expectation that emergency workers
should receive less than 5 rems would have the effect of a significant
increase in casualties among persons who could be rescued and saved if
emergency workers were permitted to do their normal
jobs.
According to Table 1, Protective Action
Guides, the public would be relocated if the projected dose in the first year
were 2 rems or subsequent annual doses after that were 500 mrem per
year. It should be noted that the average background dose on the
Colorado
plateau is 600 mrem per year, and in some areas of the world, much higher than
that. For example, in Ramasari, Iran, the average background is
about 48 rems per year_that is 4,800 mrem per year_without noticeable adverse
health effects. Forced resettlement, on the other hand, would cause many
billions of dollars in damage to the economy as well as social upheaval.
Because of widespread public fear of low-dose radiation, many people might
choose to be resettled than face such increased exposure, but persons should
not be forced to abandon their homes, personal property, and businesses based
upon unfounded fears.
The use of 2 mrem/hr as the level at
which to control access to radiation areas is unrealistically and
unnecessarily low. At a level of 0.1 rem/hr, or 100 mrem/hr, it will
take about 41 days to accumulate a dose of 100 rems, the lowest dose that is
likely to cause acute sickness, even if received instantaneously. That
calculation presumes that the dose will remain high, whereas in fact it may be
rapidly declining with time, depending upon the mixture of isotopes
used. With fallout from the detonation of a nuclear device, radiation
levels should be one-tenth of the initial level after about 7 hours (the "7/10
Rule").
Emergency workers need to have
instruments that will enable them to distinguish between 2 mrem/hr and doses
that can be quickly lethal. Instruments available at the present time
may read in microrads and be off-scale in a range when rescue operations could
be carried out with a minimal risk to the
worker.
We agree completely with the statement
in Table 1A that lack of action_due to unclear, overly complicated, or
reactive guidelines_has a high possibility of causing unintended
consequences. One reason for lack of action will be lack of appropriate
radiation monitoring instruments, or the use of inappropriate
instruments. In fact, instruments with too low a dose range may be even
worse than not having any instruments at
all.
With respect to Table 1B, we reiterate
that a dose of 100 rems is probably the lowest at which any acute radiation
sickness symptoms are to be expected. We agree that in the case of a
very serious incident such as use of an IND, incident commanders may well need to
increase the dose above the 25 rems that is suggested in Table
1B.
Finally, I would like to point out that
there is a body of work that suggests that, in small doses, radiation can have
a beneficial (so called "hormetic") effect. A "debate" on the issue was
published in the January 2005 issue of the British Journal of Radiology. The
articles, with links to numerous references, can be found online at:
http://bjr.birjournals.org/content/vol78/issue925/
One of the participants in the debate,
the late John Cameron of the University of Wisconsin (
http://www.medphysics.wisc.edu/~vrm ) makes the case for radiation
hormesis with particular clarity as
follows:
Moderate dose rate ionizing
radiation increases longevity
J R Cameron, PhD
Departments of Medical
Physics, Radiology and Physics, University of Wisconsin, Madison
WI, USA
This paper presents
little-known data to support the hypothesis that we need increased background
radiation to improve our health. Attention will be drawn to results that
demonstrate health benefits of ionizing radiation that have been largely
ignored by the news media.
Science progresses by interpreting new data
not by accepting unfounded assumptions. Arthur Conan Doyle cautioned against
making assumptions until one has enough data on which to base the assumption.
The International Commission on Radiological Protection failed to follow that
advice when it adopted the linear assumption of radiation risk in 1977,
primarily to simplify radiation protection regulations. Conan Doyle also
pointed out that a premature assumption results in a tendency to interpret
data to agree with the assumption. I believe this is one of the reasons the
linear assumption has survived for so long.
Few radiologists, or other
healthcare workers involved with radiation, are aware that billions of their
cells are bombarded daily by natural ionizing radiation, much of it from ~9
kBq of natural radioactivity in their bodies. Nearly all the trillions of
cells in our body are hit each year, many more than once. Despite this huge
amount of radiation damage, cancer is primarily a disease of the elderly. It
is reasonable to assume that our very early ancestors solved the problem of
cellular repair billions of years ago and that we now have highly efficient
repair mechanisms. Cells beyond repair undergo controlled destruction by lysis
(apoptosis). According to Cohen [1] if all cancers were curable, longevity
would only be increased by about 3 years. It is illogical to suggest that
radiation damage to one cell may cause cancer. The probability of one damaged
cell causing cancer is infinitesimal - less than ones chance of winning a
World lottery if everyone had a ticket. Scientists should not base health
effects on assumptions that cannot be proved or disproved. The linear
assumption of radiation risk was made to simplify radiation protection
regulations. It is unfortunate that many persons have accepted the assumption
as a scientific truth despite the contradictory evidence of lower cancer
mortality in high background areas.
Population
studies
There is much evidence that
radiation induction of cancer is not linear with dose and that a threshold
dose rate of the order of 1 Gy year-1 must be exceeded to induce cancer. In
addition, recent studies of radiation workers show that moderate dose rate
radiation produces a very significant reduction in death rate from non-cancer.
The increase in longevity in two studies of radiation workers was about 3
years, about equal to the increase in longevity if all cancer were curable
[2].
If ionizing radiation is as dangerous as many now believe, it
seems impossible for life to have evolved. I have suggested that ionizing
radiation may be an "essential trace energy" analogous to the many essential
trace elements we need for good health
[3].
A report by the US Atomic
Energy Commission in 1973 showed that the population in the six US States with
the highest radiation background had 15% lower cancer death rates than the
average for the 48 States [4]. In 1998 the results of this study were
confirmed by a comparison of the cancer mortality and background radiation of
three mountain States to those of three Gulf States [5]. The annual level of natural
background radiation in the three Rocky Mountain States (Idaho, Colorado and
New Mexico) is 3.2 times that in three Gulf Coast States (Louisiana,
Mississippi and Alabama), but the overall age-adjusted cancer death rate in
the Gulf States is 1.26 times higher. Thus the difference from proportionality
is a factor of 4.0.
For lung and bronchus cancer mortality there is a
strong negative correlation with natural radon levels (the main cause of the
difference in background levels) - factors of 5.7 to 7.0.
In such
studies, the possibility of confounding factors must always be considered.
However, to quote from Jagger's paper "It is possible that confounding factors
such as smoking, poverty or environmental pollution, contribute to the
differences in cancer mortality between Rocky Mountain and Gulf Coast
States. However, the
factor of disproportion is so great (4.0-7.5) that it strains credulity that
such confounding factors could reverse this negative
correlation".
Although this finding was published in a well-read
journal, it attracted no attention from the news media.
The 100-year
study of British radiologists (1897-1997) is the most important study of
health effects of moderate dose rate radiation ever published [6, 7]. It
compared the death rates of British radiologists from cancer, non-cancer and
all causes to those of all male non-radiologist physicians in
England and
Wales, hereafter referred to as
controls. The study showed that radiologists who joined a radiological society
between 1897-1920 had 75% greater cancer mortality than the controls. It is
not possible to make close estimates of doses received by radiologists at that
time. Braestrup [8] estimated average accumulated doses to US radiologists in
the 1920s and 1930s using non-protective equipment at about 1 Gy year-1 (in
modern units). 75% of the dose arose from fluoroscopy (assumed at 1 h day-1),
the remainder was equally divided between diagnostic radiography and therapy.
There is no doubt that the significant cancer increase (p<0.001) was due to
high radiation doses in those early years of radiology.
The increased
radiation had a significant beneficial effect that was not noticed at the
time. The radiologists' death rate from non-cancer was 14% lower (p<0.05)
than the controls. Their deaths from all causes were slightly less than the
controls, that is to say the longevity of the earliest radiologists was not
reduced despite their 75% increase in cancer death rate. British radiologists
who joined a radiological society after 1920 have never shown a statistically
significant excess of cancer mortality compared with the controls. This
dramatic contradiction of the linear assumption has been largely ignored. The
abrupt decrease in cancer deaths after 1920 suggests that X-ray induction of
cancer has a threshold as suggested by two earlier studies [9,
10].
With the introduction of beam collimation and personal protection,
and much later image intensifiers, doses to radiologists fell dramatically. By
the late 1950s the average had fallen to about 0.01 Gy year-1 and by the 1990s
to about 0.5 mGy year-1 [11]. The healthiest British radiologists were those
who joined a radiological society between 1955 and 1979. Their death rate from
cancer was 29% lower (not significant); from non-cancer was 36% lower
(p<0.001) and from all causes was 32% lower (p<0.001) than the controls.
Their increase in longevity over the controls is estimated to be about 3
years.
The best epidemiological
study of radiation workers ever done is the US nuclear
shipyard worker study - NSWS (1980-1988) - supported by the US Department of
Energy [12]. I was a member of the Technical Advisory Panel (TAP) that met
twice a year to review progress and to suggest improvements. TAP comprised
eight well-qualified scientists who unanimously approved the draft of the
final report of the NSWS in early 1988. It is unfortunate that the details of
this important study have not yet appeared in a peer reviewed scientific
journal. I am sure that if the results had supported the linear hypothesis of
radiation risk the details would have been published promptly. I am the
co-author of a review article on the NSWS that has not yet been accepted by a
journal [13].
The scientists who performed
the study selected about 28 000 nuclear shipyard workers with the largest
cumulative doses. They had a death rate from cancer 15% lower (p<0.01);
from non-cancer 31% lower (p<10-16) and from all causes 24% lower
(p<10-16) than 32 500 age-matched and job-matched unexposed shipyard
workers. No other study of radiation workers has had the important advantage
of job-matched controls. The very significant reduction in non-cancer deaths
is in agreement with a similar reduction of deaths from non-cancer of British
radiologists who joined a radiological society between 1955 and 1979 referred
to earlier [6]. Since the nuclear shipyard worker study had not been
published, the authors of the 100-year study were apparently unaware of the
striking similarity of the results. Neither the 100-year study of British
radiologists nor the nuclear shipyard worker study emphasised the strong
evidence that moderate dose radiation stimulates the immune system.
It
is a mystery to me why some radiologists and other healthcare workers involved
with radiation still believe that diagnostic X-ray doses much lower than
annual background radiation carry a risk of inducing cancer. None of the above
studies proves that moderate dose radiation increases longevity but they do
provide strong evidence that moderate dose radiation is beneficial to the
health. I have suggested that valuable information on this question of
longevity could be obtained from a double blind study using increased
background radiation of about 10 mGy year-1 to half of a population of senior
citizen volunteers. This dose rate is lower than that to British radiologists
in the second quarter of the last century where there was no significant
increase in cancer. I have suggested such a double blind might be carried out
in the US Gulf States where the population seems to be suffering from
"radiation deficiency"
[3].
Conclusion
The linear model is often
defended as a conservative assumption. It is not conservative if we need a
moderate dose rate of radiation to stimulate our immune system. Too little
radiation appears to result in an earlier death. The analogy would be to
reduce essential trace elements in our diet because they are poisonous in
large quantities. The great statistical strength of the studies on the
reduction in non-cancer deaths of the British radiologists and the
US nuclear shipyard workers should
not continue to be ignored.
Thank you for your
consideration,
Paul E. Morris,
M.D.
Oakland, CA
|
|
|
